As the number of Americans without any health insurance continues
to rise and health-insurance premiums escalate, once again, at double-digit
annual increases, health policy is bound to move once more to the
center of the domestic policy debate. It is a propitious time to
take stock of the nation’s health system and to explore the
options before the nation.
A. An International Perspective
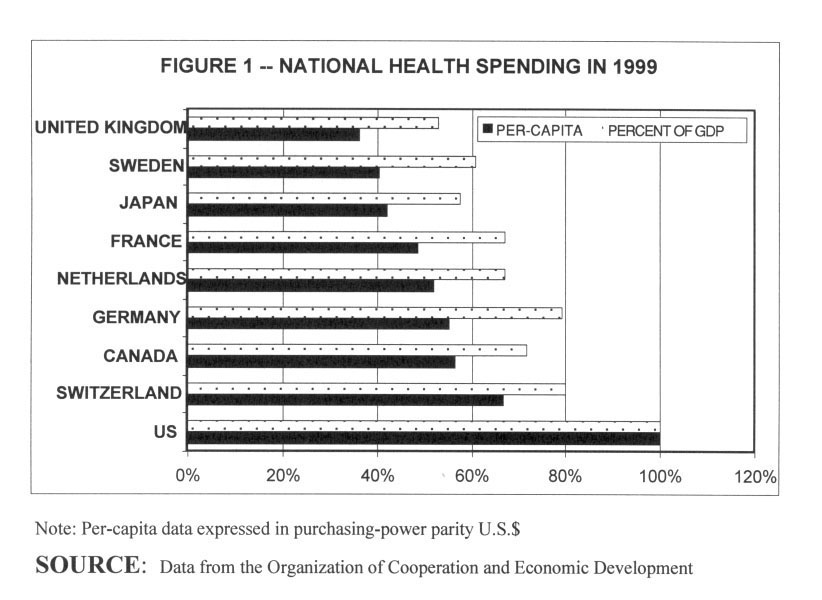
The United States has long been the most expensive health system
in the world, and it remains so today, even after a decade of "managed
care." Table 1 shows the most recent available data on total
national health spending in 1999, with the U.S. per-capita health
spending ($4,358) and U.S. percentage of GDP spent on health care
(13%) each set to 100%. The ranking for 1990 would have been quite
similar. Several points may be noted in connection with this table.
Table 1- per capita
spending and percent of GDP
Note: Per-capita data expressed in purchasing-power
parity U.S.$
SOURCE: Data from the Organization of Cooperation and Economic
Development
First, with the exception of Canada, the populations of all other
nations shown in the graph are much older than ours. To illustrate,
only in the year 2020 will the percentage of the American population
over age 65 reach the current German percentage, and only in 2025
will the American age structure reach Sweden’s current age structure.
Second, if one distinguishes between real health care services (physician
visits, hospital days, drugs, supplies, and so on) and financial resources
(spending), it is found that most of the nations shown in Table 1
actually devote more real resources overall per capita to health care
than does the U.S. The U.S. does rank higher, however, in the availability
and use of highly sophisticated medical technology.
Third, as is seen in Table 1, all other industrialized nations cede
to the providers of health care (doctors, nurses, pharmaceutical manufacturers,
etc.) a much smaller fraction of the nation’s GDP than does the
U.S. The other nations can do this because the structure of their
health insurance systems amasses monopsonistic (single-buyer) market
power on the demand side of the market , which allows third-party
payers to pay the providers of health care lower money prices for
that care than they would have to pay under the more loosely structured
U.S. system. It is the reason, for example, why prices for the same
brand-name prescription drugs can be so much higher in the U.S. than
in Canada and Europe, and why American physicians are much better
paid than their colleagues abroad. On average, the net income of American
physicians in 1999 was 5.5 times average employee compensation. The
comparable numbers for Germany and Canada are 3.4and 3.2, respectively.
Fourth, the U.S. has by far the most complex and bureaucratic health-insurance
system in the world. In an elaborate cross-national study of health
spending in 1990 published in 1996, for example, the McKinsey Global
Institute found that after all conceivable adjustments were made for
demographic and other differences between nations, Germans in 1990
spent an average $390 more on health care proper than did Americans,
while Americans spend $360 more on "administration" and
another $256 more on "other" items not specifically identified
by McKinsey, but probably including still other administrative overhead.
There simply does not exist anywhere in the world a pluralistic health
insurance system as complex, as paper hungry and as computer- and
labor-intensive as is the American system.
Fifth, on most measurable, population-based health status indicators
— e.g., life expectancy at birth or at age 65, infant mortality,
preventable years of life lost — the U.S. always has ranked and
continues to rank rather poorly relative to the rest of the industrialized
world. Neighboring Canada, whose age structure is similar to ours,
and which spends less than 60% of the comparable U.S. figure on health
care per capita, ranks higher than the U.S. on all of these indicators.
In fairness to the U.S. health system, however, it must be said that
these aggregate health status indicators are apt to reflect mainly
socio-economic influences beyond the control of the health sector
proper. Unfortunately, there is very little solid information on what
added benefits in terms of health status or personal comfort the U.S.
actually is buying with its much higher health spending. Curiously,
American policy makers and research foundations never have shown much
interest in this intriguing question. The well-endowed Robert Wood
Johnson Foundation, for example, declines to fund such research as
a matter of explicit policy.
Well-insured Americans
It probably is fair to say, on the basis of impressionistic information,
that well-insured Americans with complex diseases tend to find in
the U.S. health system more aggressive, highly sophisticated diagnoses
and medical treatments — or have speedier access to such treatments
— than might similar patients in other nations. It is one reason
why health care of this sort has become an American export that serves
a global market.
Low-income families
On the other hand, low-income families without health insurance probably
fare worse in the U.S. health system than they would in other nations.
At this time, more than 40 million mainly low-income Americans (about
7 million children among them) do not have health insurance of any
sort, a number that rose from about 35 million in 1990, as America
prospered. More than two-thirds of the uninsured are low-income, most
are members of working families, and about half have been uninsured
for two years or more.
The elderly
Between 12 to 15 million elderly Americans do not have any insurance
coverage for prescription drugs.
The uninsured
While uninsured Americans usually do receive health care for truly
critical conditions, either with their own funds or on a charity
basis, it is well known to researchers that this care is not timely
and that lack of earlier intervention can have serious consequences
for the patient (see, for example, the Kaiser Family Foundation
website www.kff.org).
Bankruptcy
Furthermore, recent research conduced by Elizabeth Warren of the
Harvard Law School suggests that medical bills are the second most
frequently cited reasons for personal bankruptcy in the U.S., right
after loss of job and ahead of divorce. Citizens in other industrialized
nations would consider it morally unacceptable to let a family stricken
by major illness go bankrupt over the medical bills.
Ethic of health care
The chronic and growing presence of the uninsured in the U.S. and
their fiscal plight suggests that different nations posit different
ethical goals for their health systems. Canadians view comprehensive
health care as a social good that should be collectively financed
and made available to all citizens on equal terms. The entire Canadians
health system is structured to serve this explicitly articulated
social ethic. By contrast, Americans have never agreed on a distributive
ethic for their health system. While some Americans do subscribe
to a purely egalitarian ethic for health care practiced in Canada,
the politically dominant, policy-making elite in the U.S. has been
content to treat health-insurance and health care as basically a
private consumption goods whose content and quality can be allowed
to vary with the individual’s income.
As every first-year student in economics is taught — or should
be taught — it is impossible to compare public policies in
terms of their relative efficiency, if those policies aim at different
social goals. Therefore, it is not meaningful to ask which nation
— e.g., Canada or the U.S. — has the "best"
health system, because the two nations posit for their systems such
vastly different social ethics. It is all a matter of taste, and,
as the Romans so aptly put it, de gustibus non est disputandum.
B. The Wondrous Roller-Coaster Ride of U.S. Health Policy
Table 2 depicts the share of health spending paid by four groups
of payers: government, private insurance, other private third-party
payer and patients, out of pocket. Some remarkable features stand
out from the display. First, the share of health spending paid out
of pocket by patients has decreased steadily over time, although
it has remained stable since 1995. Out-of-pocket spending varies,
of course, enormously among families. Second, private insurance
now covers only a third of all health spending in the U.S., over
90% of it provided by employers at the place of work. Finally, governments
at all levels combined now represent the major source of all health
spending in the U.S. If one adds to the direct government payments
shown in Table 2 the roughly $130 billion or so added taxes all
taxpayers must pay annually to cover tax-revenues lost under the
tax-preference accorded employer-paid health insurance premiums
(these premiums are not added to the employee’s taxable income),
then more than 60% of all U.S. health spending is now tax-financed.
As a percentage of GDP, tax-financed health care in the U.S. now
exceeds tax-financed health care even in the U.K., with its government-run
health system.
Table 2
- sources of U.S. health spending 1965-2000
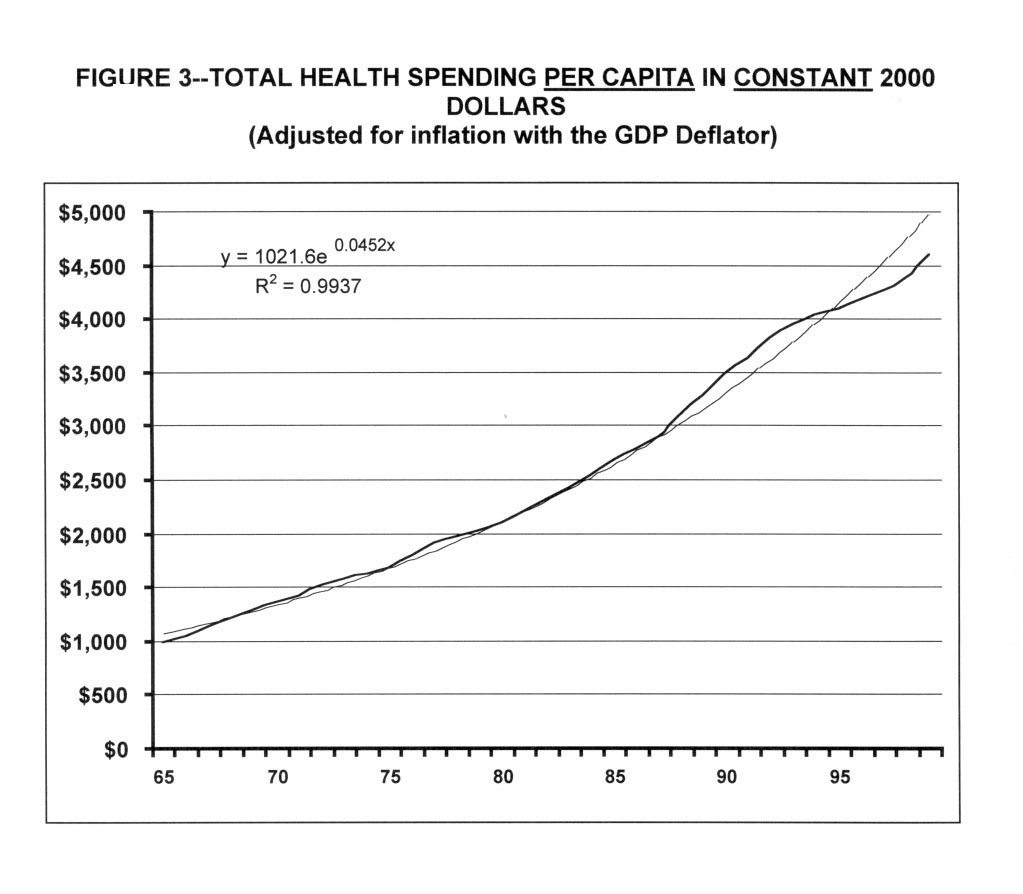
Table 2 shows the time path of per-capita U.S. health spending,
in constant (inflation-adjusted) dollars. It is seen that, from
1965 to about 1987, actual per-capita spending closely followed
a trend line according to which the health sector asked and received
from society, each year, 4.5% more real purchasing power per man,
woman and child than it did before. By contrast, constant-dollar
GDP per capita rose at a long-run average of only 1.7% per year
over the same period.
Table 3 - Total health spending per
capita in constant 2000 dollars (adjusted for inflation with
the GDP deflator)
Note: Per-captia data expressed in purchasing-power pariety
U.S. $
Source: Data from the Organization of Cooperation and Economic
Development
From 1987 on, actual spending rose above the historic trend line.
Most of the more rapid growth in spending originated in the private
insurance sector, which then still paid each doctor, hospital, and
other provider of health care more or less whatever they were billed,
with few questions asked. By contrast, for Medicare patients, the
Reagan administration had as early as 1983 imposed on the hospital
a centrally administered system of price controls that imposed a
common, uniform fee schedule for all hospitals in the entire nation.
(Were this essay not addressed to Princeton alumni, one might properly
call it a Soviet-style approach to hospital pricing). For his part,
President Bush followed suit by imposed a nationwide, centrally
set fee schedule similar with strict price controls on physicians
in early 1992, along with a total global budget for all annual Medicare
spending on physicians.
As a result of these tough price controls, Medicare spending per
beneficiary during most of the 1980s actually rose much less rapidly
than per-capita spending in the private sector. Indeed, private
insurers and the employers behind them loudly complained that the
annual premiums increases of 15% to 18% they suffered during the
late 1980s were in good part the result of a "cost shift"
from government to the private sector. The theory is that whenever
government tightly controls health spending, the providers of health
care simply increase the prices charged private payers or persuade
their patients to use added health services.
The onset of managed care
The rapid escalation of employer-paid insurance premiums, coming
as it did in the midst of the economics recession around 1990, set
the stage for the onset of what has come to be known "managed
care." At the core of this approach was the ability of private
employers, during the recession, to force upon their anxious employees
health insurance products that limited the employees’ choice
of providers to defined networks, which often limited direct access
to medical specialists, and which sometimes limited patients’
access to new and expensive medical technology — e.g., to new,
expensive brand-name medicines. Employees accepted these novel strictures
at the time, because they worried more about keeping their jobs
than about the design parameters of the health-insurance policy
that came with the job.
These limitations of choice enabled the health insurance companies
that were writing these policies to contract selectively with physicians,
hospitals, pharmacies, and other providers for the health care owed
the insured. Selective contracting, in turn, converted these providers
of health care into fiscally dependent subcontractors of particular
health plans. The plans could impose serious fiscal hardship on
individual providers, simply by canceling their contracts with the
plan. That fiscal dependence, and the constant economic threat it
implied, enabled the health plans to extract from the providers
of health care steep price discounts. It also enabled the health
plans to impose upon providers clinical practice guidelines that
determined whether or not a health plan would pay for particular
services rendered. Altogether, these novel relationships among insurance
plans, on the one hand, and the providers of health care and their
patients, on the other, constituted the phenomenon properly called
"managed care."
As is shown in Table 3, the attempt to control
American health spending through the techniques of "managed
care" did bend the time path of actual real per-capita health
spending during the period 1992-97 below the long-run spending trend
line. During the mid 1990s, real per-capita health spending rose
at rates much below the historical long-run average of 4.5%. The
health insurance premiums charged employers for their group policy
rose at ever smaller annual rates, reaching an average of a zero
increase in 1996. The percentage of GDP spent on health care was
virtually constant, hovering about 13.5%. In 1993 Congressional
Budget Office (CBO) had projected that health spending in the year
2000 would be $1.67 trillion, or close to 20% of the GDP. The actual
number for 2000 turned out to be $1.3 trillion, or only about 13%
of GDP.
Economic theory suggests that, in the tight labor markets of the
1990s, the bulk of these savings in health spending are likely to
have flown through to employees in the form of higher take-home
pay. That theory, however, is not widely shared among non-economists.
A more popular theory in the press, and especially among the providers
of health care, is that these savings reflect the denial of needed
care to the insured and that they flowed mainly into the bottom
line of employers and the paychecks of health insurance executives.
The "managed care" backlash unleashed by physicians, politicians,
and the media was driven by this popular theory.
Starting in 1997, with "managed care" in wholesale retreat,
overall average real per capita health spending in the U.S. has
been rising once again, at an ever-accelerating pace. As is seen
in Table 1, it now proceeds at roughly the
same high growth rate that was experienced during the late 1980s—albeit
still below the long-run historical trend line. For the 2001-2002
season, these increases are projected to be in the mid- to high
double digits, even for large employers, and in excess of 20% for
small employers and individuals.
Per capita health spending under the public Medicare and Medicaid
programs currently are still rising at much lower rates than those
in the private sector, partly as a result of cost-control measures
legislated in the late 1990s. It is only a matter of time until
these public programs must adapt to the prices and spending levels
set by the private sector. Furthermore, just as in the later 1980s,
private insurers and employers are convinced once again that the
tighter control of government health spending shifts costs to private
payers. Therefore, they will lobby the Congress to relax the reins
on public health spending. In short, the health-care cost crisis
of the late 1980s has returned to the U.S. in full bloom.
C. The next few Years in U.S. Health Policy
During the course of the past two decades, the legendary American
voter, has spoken clearly articulated the preferred health policy.
That legendary voter is worried about the cost of health care and
about losing health insurance coverage. Utterly convinced by TV
actors Harry and Louise that government ought not to introduce into
something as delicate as health care, however, the U.S. voter prefers
a private health insurance system. The voter does, of course, expect
private insurers to control the cost of health care, but not through
controls over the volume of health care, nor through downward pressure
on prices.
Volume controls represent "rationing," which is un-American,
at least insofar as insured Americans are concerned. Downward pressure
on the for prices hospital care is known to lead to nursing shortages
and hence reduce the quality of care. Downward pressure on physician
fees is known to detract from the quality of physician care, as
doctors are forced to defend their income by processing more patients
more quickly. Price controls of prescription drugs are known to
inhibit research and development by that industry.
In short, the American voter wants (1) instant access to (2) affordable
health care in a system that (3) controls health spending through
something other than prices or volume. To thoughtful persons, that
wish list poses a challenge. Indeed, to thoughtful persons, the
aspirations of the American voter in matters of health policy are
so young, to put it politely, that serious policy makers have long
despaired of taking voters’ aspirations seriously.
Health policy in this country therefore has been and is being forged
strictly among a narrow policy-making elite that could easily fit
into the Grand Ballroom of the Washington Hilton hotel. Within that
elite, there has been a decade-long, tenacious fight between two
distinct camps: the egalitarians, who would like to see health care
run on a social contract such as Canada’s, and the libertarians,
who view health care as a private consumption goods whose quantity
and quality can properly be rationed by the individual’s income.
During the debate over health reform in the early 1990s, for example,
Nobel Laureate economist Milton Friedman proposed the complete abolition
of the federal Medicare program for the elderly and the state-federal
Medicaid program for the poor. Instead, he advocated that families
have only catastrophic health insurance, with an up-front, out-of-pocket
deductible of $20,000 per year or 30% of the family’s income
during the last two years, whichever is lower (The Wall Street
Journal November 12, 1991). At the time of his writing, the
median pretax family income in the U.S. was $35,000, which means
that he had in mind a $10,500 deductible for such a family.
It appears that the libertarians are winning this contest. As national
health spending rises once again annually at double-digit rates,
the insurance industry is poised to segment its clientele more and
more by actuarial risk class, that is, by health status. It is achieved
through the process of computer-based "mass customization"
that allows insurers to tailor a family’s health insurance
policy ever more closely to its own "needs" — code
for "actuarial risk" or "health status." Many
of these new insurance products will be patterned on Milton Friedman’s
vision. Eventually, the Medicare program will move in this direction
as well. The net economic effect of these developments will be to
allocate less of the financial burden of health care to the chronically
healthy, who "consume" relatively little health care,
and more to the chronically sick, who "consume" relatively
more.
On the back of these trends, the health care system of the future
in the U.S. is likely to fall into at least four distinct tiers,
with the following offerings, by income class:
1. For the millions of uninsured who are unlikely to be covered
in this decade, if ever, under the emerging tight government budgets,
whatever they can afford with their budgets or can scrounge up as
health-care beggars from kindly doctors and hospitals.
2. For Medicaid beneficiaries and low-income employees in
firms that do offer employees health insurance, tightly managed
Health Maintenance Organizations (HMOs) that will seek to limit
choice and ration health care judiciously, in accordance with guidelines
and the premiums they are paid.
3. For middle- and upper income employees, mild if any rationing
and wider choice of provider and therapy under the so-called Preferred
Provider policies (PPOs) which will, however, charge higher premiums.
4. For very high-income people — executives prominent
among them — open ended indemnity policies without any limit
on choice and without any form of rationing—the perfect clientele
for boutique medicine.
There will of course be sundry tiers in between.
This is not a futuristic vision. The system is already in place,
albeit by happenstance and default. The difference will be an income-based
system will be more formally more formally and officially sanctioned
by the Congress and the state legislatures of the United States.
It would as yet remain politically incorrect to advocate such a
system explicitly.