The onset of inflammation and infection in a person recovering from a trauma such as a car accident or severe burns can be as deadly as the incident itself. New findings from Princeton University researchers who studied gene activity in trauma victims may help to predict and better treat such unexpected complications.
Princeton research reported in the Sept. 13 issue of the journal PLoS Medicine shows for the first time that people recovering from a serious injury -- regardless of age, gender or previous health -- exhibit similar gene activity as their condition changes, which doctors can use to predict and prepare for a patient's deterioration.
The Princeton researchers' evaluation of blood samples from 168 blunt-force trauma patients revealed that changes in gene activity -- or expression -- in the immune system consistently coincided with the worsening of a patient's condition. Immune system genes "express" via an outpouring of proteins to help activate and direct the cellular response to injury and viruses, bacteria or other pathogens. Two sets of genes in particular showed massive fluctuations in expression as patients developed complications and neared death.
After the researchers identified the genes that were most in step with a patient's state of health, they created a model based on gene expression that could help physicians better evaluate and treat critical patients.
"Plenty of genes were changing inside these patients as their bodies adjusted to the trauma they experienced, but we wanted to find the genes that, over time, foretold the outcome for the patient," said senior author John Storey, a Princeton associate professor of molecular biology and the Lewis-Sigler Institute for Integrative Genomics. He worked with the PLoS Medicine paper's joint first authors Keyur Desai and Chuen-Seng Tan, both postdoctoral research fellows in Storey's lab.
"We started this project three years ago with approximately 50,000 documented gene expressions in these patients," Storey said. "We were amazed to see that as the list of genes directly related to a patient's health became smaller, the biological picture became clearer and we could pinpoint specific pathways. It was startling to see something so clean emerge from a study with so many variables."
Princeton molecular biologist John Storey (left) and postdoctoral research fellow Keyur Desai analyzed the gene activity of a 168 blunt-force trauma patients and found that it correlated with a patient's deterioration. The Princeton work is the latest from a 10-year, $100 million federally funded project based at Massachusetts General Hospital to examine the genomic causes of why people experience different outcomes to similar injuries. (Photo by Denise Applewhite)
The search for the genomic response to trauma
The Princeton findings are the latest to stem from a 10-year, $100-million effort to unravel the genomic underpinnings of why people experience vastly different outcomes to similar traumatic injuries. Based at Massachusetts General Hospital, the Inflammation and the Host Response to Injury (IHRI) project brought together more than 60 researchers from 22 U.S. universities and medical centers. The IHRI consortium studied 1,977 severely injured and burned patients at U.S. trauma centers from 2003 to 2011, and the Princeton researchers worked with data from 168 of those patients enrolled in the first five years of the study. The National Institute of General Medical Sciences, a division of the National Institutes of Health, funded the project through its Large Scale Collaborative Projects, or "Glue Grant," program.
The work conducted at Princeton produced one of the project's most significant findings -- that at the genetic level, the human immune system is in fact very consistent from person to person -- said Ronald Tompkins, the IHRI project's principal investigator and a co-author of the PLoS Medicine report.
Conventional medical wisdom has long held that the reason a horribly injured 20-year-old is released from the hospital after seven days, while a 65-year-old with similar injuries eventually dies, is because the basic elements of their immune systems are completely different, said Tompkins, who is the chief of burns service at Mass General and a professor of surgery at Harvard Medical School. That assumption makes complications hard to predict and manage. Desai, Storey and Tan, however, have shown that immune responses can be foreseen in the universal activity of genes, Tompkins said.
"There are going to be differences due to mutations, but the general systems operate in a nearly identical fashion from person to person," Tompkins said. "This paper is the first to really identify that the differences in genomic response are quantitative. The systems of the young patient versus the older patient are qualitatively identical. The degree with which the genes regulate up or down might be less and deviations might return to normal more quickly or slowly. But there are no new genes or pathways to recruit, and the direction of regulation is the same in both."
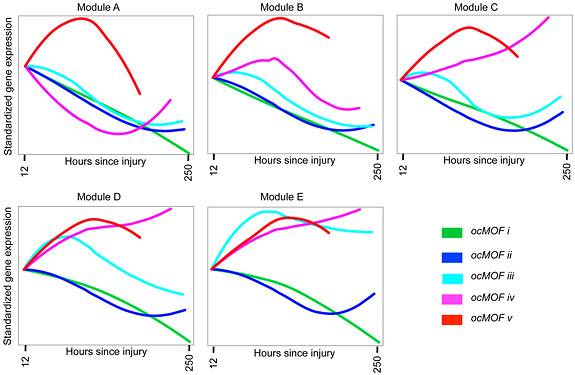
The Princeton researchers produced a model that physicians could use to determine trauma patients' chances of survival based on their gene activity. Each module correlates activity for a specific gene family with the patient's possible outcome (colored lines), which is based on the likelihood of death; all patients categorized as ocMOF v (red) eventually died. A physician would determine the outcome indicated by each gene family, then combine those observations to identify the overall chances of survival. (Image courtesy of John Storey, Keyur Desai and Chuen-Seng Tan)
Erratic immune response: 'That's why they die'
The Princeton researchers analyzed data on patients who had been observed for 28 days by other researchers involved in the IHRI project and whose health status had been documented through almost 400 clinical variables describing the patients' condition. As part of the effort to better understand the genomic activity of these trauma victims, Stanford University researchers involved in the project analyzed blood samples to create a profile of white-blood-cell gene expression for each patient.
Using this data collected by the Stanford researchers, the Princeton team first created a system to classify each patient's condition. Tan used documentation of the patients' condition and prognosis to develop five distinct categories based on the likelihood of death from multiple organ failure -- all patients in the fifth category eventually died. At the same time, Desai condensed the mass of gene data into a scale illustrating how each gene's expression changed over time for each patient.
Storey and his colleagues used these scales to identify which genes exhibited the greatest change in expression as a patient's health degenerated. They narrowed the initial 50,000 expressions to the top 3,000 gene expressions associated with a patient's condition.
A second whittling of the list -- this time to the top 500 health-related gene expressions -- exposed two sets of genes whose activity presaged patient outcome within 40 to 80 hours of the injury. MHC-class II genes -- which recognize infection-fighting proteins known as antigens and transport them to the surface of specialized cells that then carry out the immune response -- showed decreased expression as a patient worsened. At the same time, the expression of genes known as p38 MAPK that help trigger inflammation and swelling -- part of the body's immune arsenal -- clearly spiked.
Combined, these observations suggest that trauma patients who eventually die develop an erratic and paradoxical immune response, Storey said.
"Perhaps that's why they die," he said. "The patients in our fifth category had mass inflammation that wreaked havoc on their organs because p38 MAPK was turned up, but the genes that recognize and help fight pathogens, MHC-class II, were turned down."
Using the set of 3,000 gene expressions, the Princeton researchers created a model intended to help doctors correlate genomic activity with health status. The model resembles the methods used to diagnose conditions such as heart attacks by determining the severity of various factors, Storey said. The model is composed of five separate graphs, with each one correlating expression patterns in a specific gene family to the five categories of patient conditions based on likelihood of death that the researchers previously established. The model is set to a timescale of 12 hours to roughly 10 days following injury.
The model shows, for example, that if one family of genes exhibits a jump in expression early on, the patient's condition might be in the deadly fifth category; however, if activity for those same genes diminishes quickly, the patient could experience a good outcome. The same determination is made for each of the five graphs of gene expression patterns to establish the patient's overall risk of infection and death.
"We wanted something a doctor could use in the clinical setting to ascertain a patient's condition," Storey said. "The way to do that was through a model that is incredibly simple and a straightforward depiction of natural processes.
"With the amount of data we started with, we struggled for years before we realized that this type of model was the way to go," Storey said. "It wasn't obvious, and our inclination was to produce a complicated model of all gene expression. It was similar to using simple tools to fix a car when the temptation is to rebuild the engine. But the simple tools worked very well."
That simple tool -- a practical clinical model fashioned from reams of expression data -- is a significant step toward using genomic analyses to directly treat patients, said Stephen Friend, president of Seattle-based Sage Bionetworks, as well as a biochemist and physician. Friend, whose company supports and assists with genomic research with clinical applications, had no role in the Princeton research, but he is familiar with it.
In the past five years, genomic profiles of patients have become commonplace in commercial and academic clinical trials, Friend said. When it comes to treatment, however, the application of genomics is not as widespread. One reason is that the advantage of monitoring a patient's gene expression -- namely that thousands of health markers can be identified through genetic activity -- also results in a problematically large dataset, as the Princeton researchers encountered.
"Their work shows a logical way to tame those tens of thousands of variables and put them in a practical, insightful guide that a clinician can use," Friend said.
"What's more important is that the Storey group applied genomics to an area that really needs it. They ordered patterns of expression in an elegant way that would allow this information to be parsed into particular decisions that would guide clinical care. This kind of work is precisely what is needed to extend the use and benefits of genomics data to practical day-to-day use in the clinic."
'It's like a massive explosion'
The work from Storey's group finally organizes what is known about post-trauma inflammation in a way that was necessary to treat the condition, said co-author Ronald Maier, a surgeon and professor at the University of Washington School of Medicine who oversaw and coordinated the clinical portion of the IHRI project.
Previous research has shown that about two-thirds of gene sets spring into action in severe trauma patients, making the immune response so overactive and prolonged that it can be deadly. The Princeton researchers have provided a method for discerning from the flood of gene expressions the activity that is central to complications, he said.
"Evolution did not plan on survival in a surgical intensive-care unit," Maier said. "These patients are so injured and the response is so massive that it becomes autodestructive. It's like a massive explosion. It's a constantly changing process, so you can imagine trying to track 15,000 proteins that change over time. This work comes in by introducing a new technique to handle this massive amount of data."
In addition, the Princeton researchers have identified potential drug targets for controlling the immune response that leads to inflammation, Maier said. Past attempts to restrain this reaction have failed due to the complex relationship existing between the thousands of genes and proteins, he said. Experimental drugs focused on specific genes and proteins, sometimes eliminating what turned out to be crucial players and upsetting the system even more, he said.
"In retrospect, approaches to this problem may have been somewhat naive," Maier said. "There are thousands of proteins, and fixing one or two of them is unlikely to have an impact. The benefit we want from the IHRI is to use the genes most tightly linked to patient outcome to develop targeted intervention and drug therapy.
"This work provides the mathematical model to understand the body's extreme response to trauma -- the job now is to come up with mechanisms to safely control it."

